With over 1200 messages in my personal e-mail Inbox… you can say that we are drowning in data! Many of those e-mails are less than helpful for the cause… with the COVID-19 pandemic, many bureaucratic bodies are sending out daily (sometimes 2 and 3 times a day!) messages. All attempting to inform when in actual fact, they are creating too much distracting noise.
Now that we have switched to a significant increase in telemedicine (see April 8th post Marvelous Mental Health) via telephone, text, e-mailing/sharing pictures and video visits… I think patient-centred care has taken a positive step forward in all of this COVID-19 innovative #physicaldistancing and flattening the curve work!
Unfortunately, with providing this increase in comprehensive and quality relational medical care, the boundaries of where and when we do Family Medicine are blurring big time (we’ll leave the time consuming Electronic Medical Records (EMR) data entry for another time ;D).
I am getting calls, texts and messages late in the evening and on weekends (even during my #lockdown holiday). As a Family Doctor, it is hard to “just say no” when you know sometimes that care is compromised when you don’t answer the call… especially during this global pandemic when we want to keep patients and the public safe.
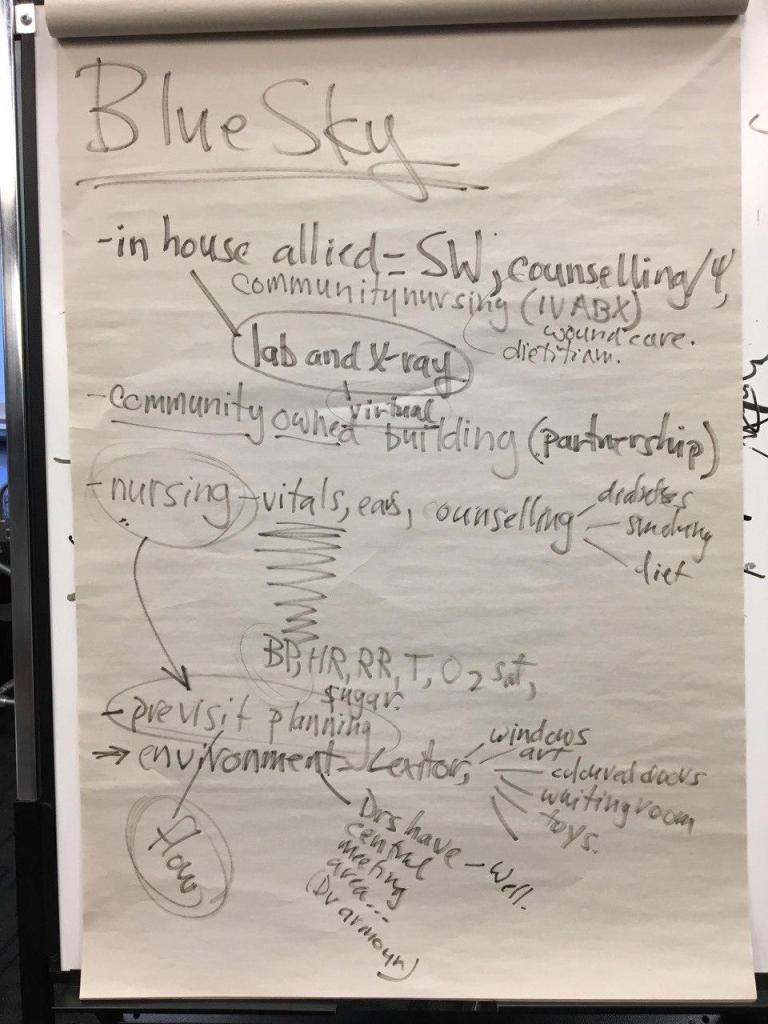
I admit that I am still working on my personal e-boundaries here, but want to acknowledge that with the Blue Sky Family Medicine model, it will be the triad and quad of Family Doctors which will be a game changer in the future (can you say Orange Leader?)… we are currently beta testing and perfecting it!
I found this book review by Nina Semczuk on Cal Newport’s book Digital Minimalism very helpful with establishing healthier and more fuctional e-boundaries:
As we continue to innovate and improve how we deliver high quality Family Medicine in Nanaimo, I have found the phone counselling visit (13038) to be over the top helpful for patients (and myself)!
Many patients who have ongoing Mental Health issues like Anxiety and Depression are challenged with easy access to counselling and relationship-based longitudinal care. As a Family Doctor who has a special interest in improving Mental, Physical and Spiritual Health, I have found this to be a key ingredient!
Relationships heal!
Here is some sage wisdom from Nanaimo psychiatrist, Dr. Joris Wiggers:
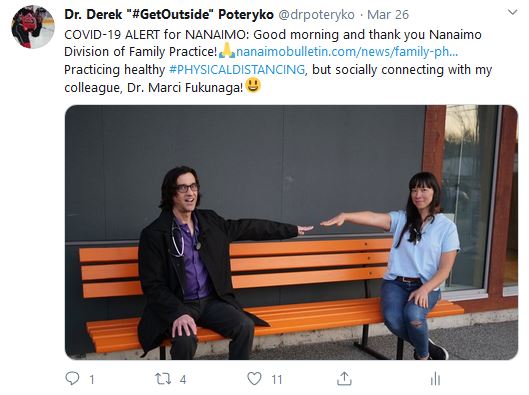
Amidst a global pandemic, we continue to help and heal our patients in Nanaimo. We have switched to telephone and/or virtual visits. This can occur 85% of the time with few face to face encounters in office to help protect patients and staff from COVID-19 spread (can you say #PhysicalDistancing?).
Anchor waiting room (notice chairs)
This innovation alone is a game changer and is helping transform Family Medicine for the better!
From a Mental Health perspective, our reach to those patients suffering from depression, anxiety and addictions has been noteworthy – counselling and treatments are started in a more thoughtful and proactive manner (#RelationshipsHeal)!
We will continue to update as we go along and remember: you are not alone and we are all in this together.
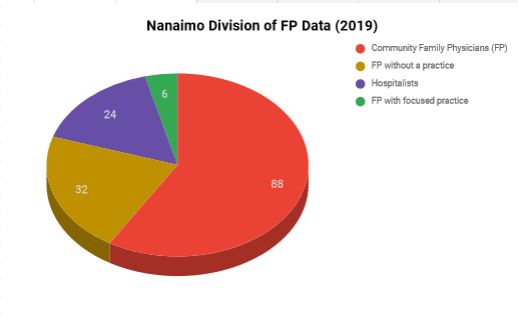
… not working in community Family Practice (FP) clinic settings. Since 2009, about half of all of the graduates from the UBC Family Practice Residency program (Nanaimo site) have chosen to remain and live in Nanaimo!
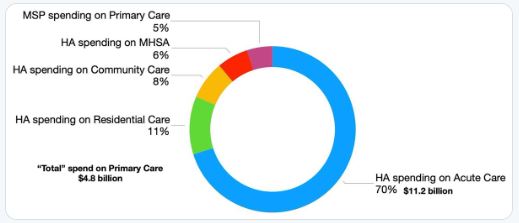
It is complicated, but community resource allocation for Primary Care (vs Acute Care) is a major cause of this paradox.
Acute Care vs Primary Care spending in B.C.
In October 2019, this information was shared with Nanaimo City Council. Dr. Poteryko, shared the 6 E’s to better Health.
The 7th E will be shared in an upcoming Episode III
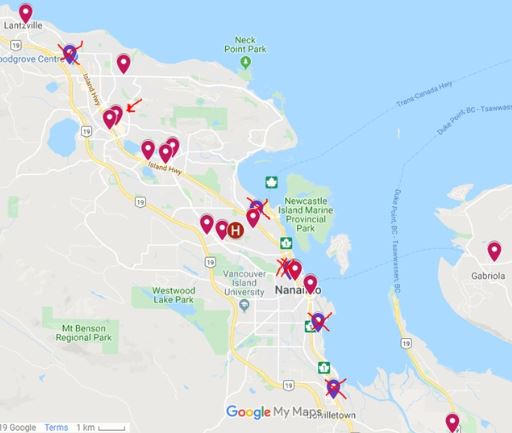
In 2017, Dr. Steve Beerman with other community Family Physicians co-wrote Primary Care Plus which was an innovative plan to revitalize community Family Practice for Nanaimo. It was supported by the Nanaimo Division of Family Practice and Island Health only to be dismissed by the Ministry of Health. This plan would have averted some of the recent closures of community Family Practice clinics in Nanaimo (since April 2018, 6 clinics have closed – see X’s below).
Nanaimo Family Physician Clinics (closures X)
Currently, there are over 21,000 people who do not have a Family Physician or other primary care provider (NP or NiP) in Nanaimo. Primary Care Plus which has now evolved into Blue Sky Family Medicine will redefine and revitalize Primary Care in Nanaimo for good. This blog will be the ever-evolving blueprint for this ideal, blue sky way of helping and healing.
Being a Family Doctor or Family Physician (FP) is not Greek to me!
Four Principles of Family Medicine
1. The family physician is a skilled clinician.
Family physicians demonstrate competence in the patient-centred clinical method; they integrate a sensitive, skillful, and appropriate search for disease. They demonstrate an understanding of patients’ experience of illness (particularly their ideas, feelings, and expectations) and of the impact of illness on patients’ lives.
Family physicians use their understanding of human development and family and other social systems to develop a comprehensive approach to the management of disease and illness in patients and their families.
Family physicians are also adept at working with patients to reach common ground on the definition of problems, goals of treatment, and roles of physician and patient in management. They are skilled at providing information to patients in a manner that respects their autonomy and empowers them to “take charge” of their own health care and make decisions in their best interests.
Family physicians have an expert knowledge of the wide range of common problems of patients in the community, and of less common, but life threatening and treatable emergencies in patients in all age groups. Their approach to health care is based on the best scientific evidence available.
2. Family medicine is a community-based discipline.
Family practice is based in the community and is significantly influenced by community factors. As a member of the community, the family physician is able to respond to people’s changing needs, to adapt quickly to changing circumstances, and to mobilize appropriate resources to address patients’ needs.
Clinical problems presenting to a community-based family physician are not pre-selected and are commonly encountered at an undifferentiated stage. Family physicians are skilled at dealing with ambiguity and uncertainty. They will see patients with chronic diseases, emotional problems, acute disorders (ranging from those that are minor and self-limiting to those that are life-threatening), and complex biopsychosocial problems. Finally, the family physician may provide palliative care to people with terminal diseases.
The family physician may care for patients in the office, the hospital (including the emergency department), other health care facilities, or the home. Family physicians see themselves as part of a community network of health care providers and are skilled at collaborating as team members or team leaders. They use referral to specialists and community resources judiciously.
3. The family physician is a resource to a defined practice population.
The family physician views his or her practice as a “population at risk,” and organizes the practice to ensure that patients’ health is maintained whether or not they are visiting the office. Such organization requires the ability to evaluate new information and its relevance to the practice, knowledge and skills to assess the effectiveness of care provided by the practice, the appropriate use of medical records and/or other information systems, and the ability to plan and implement policies that will enhance patients’ health.
Family physicians have effective strategies for self-directed, lifelong learning.
Family physicians have the responsibility to advocate public policy that promotes their patients’ health.
Family physicians accept their responsibility in the health care system for wise stewardship of scarce resources.
They consider the needs of both the individual and the community.
4. The patient-physician relationship is central to the role of the family physician.
Family physicians have an understanding and appreciation of the human condition, especially the nature of suffering and patients’ response to sickness. They are aware of their strengths and limitations and recognize when their own personal issues interfere with effective care.
Family physicians respect the privacy of the person. The patient-physician relationship has the qualities of a covenant – a promise, by physicians, to be faithful to their commitment to patients’ well-being, whether or not patients are able to follow through on their commitments. Family physicians are cognizant of the power imbalance between doctors and patients and the potential for abuse of this power.
Family physicians provide continuing care to their patients. They use repeated contacts with patients to build on the patient-physician relationship and to promote the healing power of interactions. Over time, the relationship takes on special importance to patients, their families, and the physician. As a result, the family physician becomes an advocate for the patient and family.
family – A group of people, usually of the same blood (but do not have to be), who genuinely love, trust, care about and look out for each other. Not to be mistaken with relatives sharing the same household only.
Family Medicine, it’s what we love and are honoured to do!
i’m a doctor, but i’m not a specialist or just a gp and i don’t bill mocap.
i take care of patients, not clients
i am not a hospitalist, but i see patients in the hospital
i am not an obstetrician, but i delivered babies
i am not a pediatrician, but i take care of children
and i am not a geriatrician, but i take care of the elderly
from womb to tomb care is the what i do
as a professional, i can care for 90% of what 90% of patients need clinically, anywhere, anytime and off hand, I don’t know what Muckle-Wells syndrome is, but i know how it would impact my patient and their family
i am a scholar which means i’m a lifelong learner
i am a manager, but most importantly a caring clinician and not a gatekeeper
i believe in shared care
as a communicator, i speak to my patient, their families, specialists and other healthcare professionals and
i am an advocate for my patient’s health care needs.
and i collaborate with RN’s, LPN’s, MOA’s and other healthcare professionals (like NP’s!) – they are all truly amazing people and an integral part of our healthcare system
and without them we’d be lost… i said lost!
i believe it is relationship which facilitates healing
i connect, support and empathize
i give compassionate, continuous and comprehensive care
i am the expert in managing the complexity of my patient’s medical needs,
while i prevent harm, prevent disease, and minimize suffering. as family physicians, we are the largest body of doctors in canada
still the 1st nation in hockey!
and the best part of medicine!
my name is derek and i am a canadian family physician…
André Picard is a health reporter and columnist for The Globe and Mail, where he has been a staff writer since 1987. I have been reading and following him for a few years now. He has an excellent perspective of the Canadian healthcare system.
Scientist and Family Physician for over 20 years living and learning in Nanaimo, B.C., Canada. All ideas and tweets are mine – they do not represent the organizations I am affiliated with.
We started the New Year off right in Nanaimo Regional General Hospital (NRGH) today. It was the inaugural shift for the GP in Hospital (GPIH) or Family Doctor of the Day (FDOD) program. My colleague, KW (thank you!), bravely went where no community FP has gone before… more on this later.
Relational medicine in hospital took a positive step forward in our community.
With community Family Medicine in a downturn, right now… it is our hope to help rebuild and revitalize this lost art (and science). This blog will help chronicle some of those teachings/learnings, innovations and improvements (can you say rough draft for an upcoming textbook?).
Hoping that everyone has a healthy and happy 2020!